Basics of Treatment
Full work up is performed for any patient with a mass concerning for head and neck cancer. This typically includes:
- Imaging with CT Neck and Chest with consideration for PET/CT after positive biopsy
- Direct Operative Laryngoscopy for tumor mapping and biopsy
- Dental evaluation for potential radiation therapy
- Any appropriate medical workup for optimization prior to treatment
- Treatment recommendations are typically decided on by a multidisciplinary tumor board with use of NCCN guidelines
Once diagnosis is obtained, staging is then assigned based on AJCC 8.
Scroll to continue
Laryngeal/hypopharyngeal cancer stage dictates type of treatment. Over the past several decades there has been a move towards organ preservation-based treatment which allows patients to maintain quality of life as well as oncologic outcomes.
Multidisciplinary Tumor Boards (MTBs)
All patients who are diagnosed with a new head and neck cancer should be presented at a multi disciplinary tumor board.
Head and Neck Multidisciplinary Tumor Board consist of practitioners from different specialities and can include:
- Head and Neck Surgery
- Medical Oncology
- Radiation Oncology
- Radiology
- Pathology
- Oral Surgery
- Speech Language Pathology
- Nurse Navigator

Multidisciplinary Tumor Boards (MTBs)
Patients discussed at MTBs have:
- Better stage classification
- Improved adherence to standard of care treatment
- Higher rates of treatment
- Shorter interval time to treatment
- Improved cancer outcomes
Prades J, Remue E, van Hoof E, Borras JM. Is it worth reorganising cancer services on the basis of multidisciplinary teams (MDTs)? A systematic review of the objectives and organisation of MDTs and their impact on patient outcomes. Health Policy. 2015;119(4):464–7.
Specchia ML et al. The impact of tumor board on cancer care: evidence from an umbrella review. BMC Health Services Research 20, Article number: 73(2020).
Typical treatments based on stage at diagnosis for laryngeal and hypopharyngeal cancer:
Stage I
Stage I can be treated with either radiation or surgery.
Stages II & III
Stage II and III are typically treated with radiation-based treatment for organ preserving therapy. Chemotherapy is typically added for Stage III.
Stage IV
Stage IV cancers are most often treated with total laryngectomy followed by radiation therapy for those who are surgical candidates. Chemotherapy is added for patients with high-risk pathological features.
Prognosis
Survival has improved over the past several decades for patients with laryngeal cancer.
However, survival does decrease dramatically with both regional and distant spread of disease.
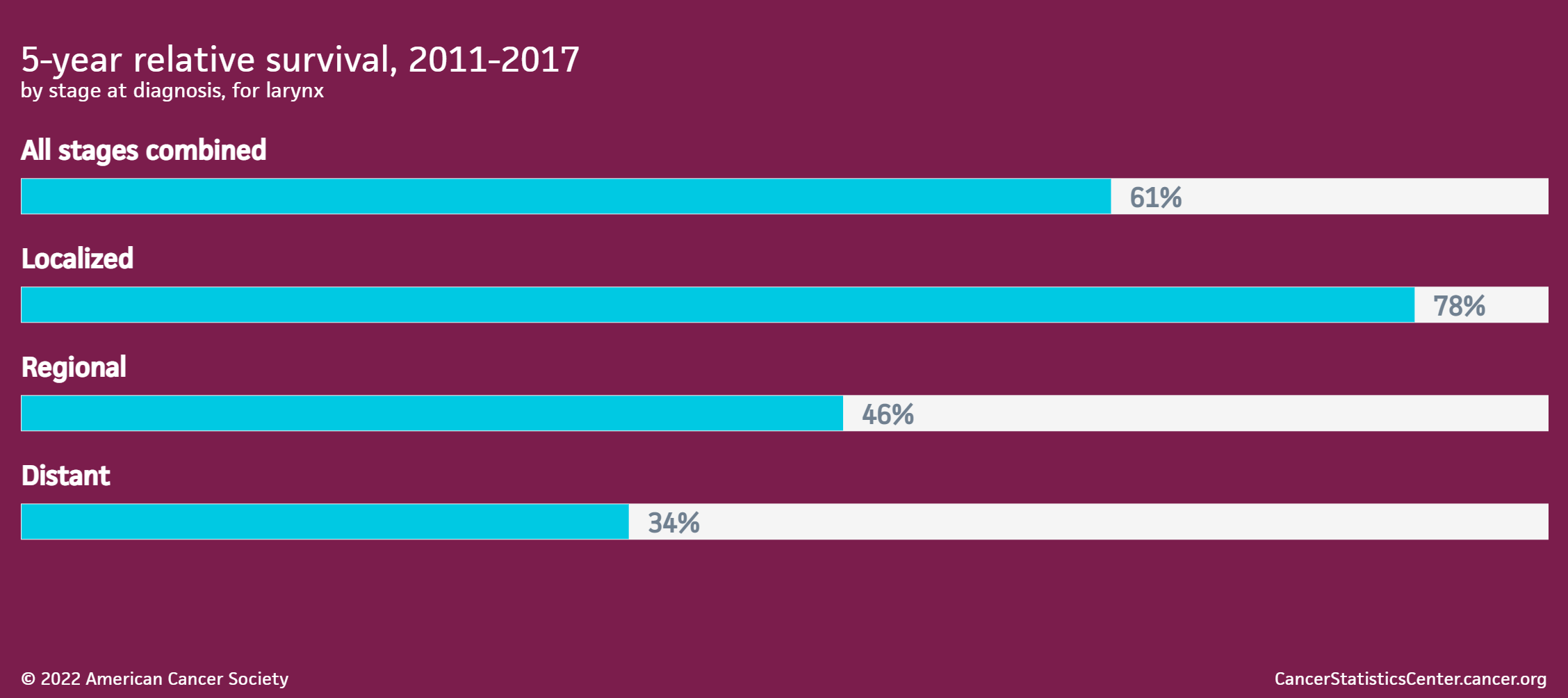
Source: https://cancerstatisticscenter.cancer.org/#!/cancer-site/Larynx
Head and Neck Cancer Survivorship
- The National Comprehensive Cancer Network (NCCN) recommends integration of primary care in survivorship care within 1 year of completion of treatment, complementary to the oncology team
- Patients should be referred for tobacco and alcohol cessation as needed
- Assess for distress, depression and/or anxiety at regular intervals
- Evaluate for thyroid dysfunction every 6 to 12 months, particularly with prior neck irradiation
- Consider chest CT as clinically indicated for those with a smoking history
Continue to: